
Pilonidal cyst treatment with the EPSIT technique — same-day discharge, rapid return to daily life. Over 300 procedures performed, patients from 4 continents.

A pilonidal cyst is an inflamed cavity that forms in the intergluteal cleft — the space between the buttocks, near the coccyx. Inside this cavity, hair, cellular debris, and bacteria accumulate, creating an environment prone to recurrent infections.
The word "pilonidal" comes from Latin: pilus (hair) + nidus (nest). Literally, a "nest of hair" beneath the skin.
The cyst may present as a painful lump, an abscess with discharge, or one or more openings in the skin that drain continuously. In many cases, the condition is chronic — with episodes of inflammation, drainage, and apparent improvement that repeat over months or years.
A pilonidal cyst does not resolve on its own. Without proper treatment, it tends to worsen.
Localized pain between the buttocks that worsens when sitting, walking, or during physical exertion. It can range from mild discomfort to intense, debilitating pain.
A palpable protuberance or lump in the area, often reddened and warm to the touch — signs of active inflammation or abscess formation.
Drainage of purulent, yellowish, or blood-tinged fluid through one or more openings in the skin. The discharge may have an unpleasant odor and stain clothing.
Small "holes" or depressions along the intergluteal cleft — these are the external openings of the cyst's fistulous tracts.
During acute episodes (abscesses), there may be fever, chills, and a general feeling of illness.
The most frustrating pattern: cycles of inflammation, spontaneous drainage, temporary relief — and then it all starts again. Many patients live with this cycle for years.
If you experience intense pain, high fever, or abundant discharge, seek immediate medical attention.
Without proper treatment, a pilonidal cyst can progress from an uncomfortable condition to a serious problem.
Acute infections requiring emergency drainage, with intense pain, fever, and inability to sit or work.
The cyst branches out, creating tunnels under the skin that open at multiple points. Treatment becomes progressively more complex.
Constant drainage of purulent discharge with an unpleasant odor, causing severe impact on self-esteem and social life.
The infection can spread to adjacent tissues, significantly worsening the clinical condition.
Medical literature documents malignant transformation (squamous cell carcinoma) in long-standing chronic cysts — although exceptionally rare.
Lost work days, embarrassment in intimate situations, anxiety and depression related to the chronic condition.
EPSIT stands for Endoscopic Pilonidal Sinus Treatment. It is a minimally invasive technique developed in Europe that uses an instrument called a fistuloscope to visualize and destroy the cyst from the inside out, without the need for external skin incisions.
The fistuloscope is only 3mm in diameter — thinner than a coffee straw. It contains a high-definition camera, an integrated working channel for surgical instruments, and a continuous irrigation system. The entire procedure is performed under direct vision on a video monitor.
Duration: 20 to 45 minutes | Anesthesia: spinal or sedation with intraoperative pain control
The 3mm fistuloscope is inserted through the external opening. Under continuous irrigation, the surgeon visualizes the entire extent of the fistulous tract in real time — identifying branches, cavities, and internal openings.
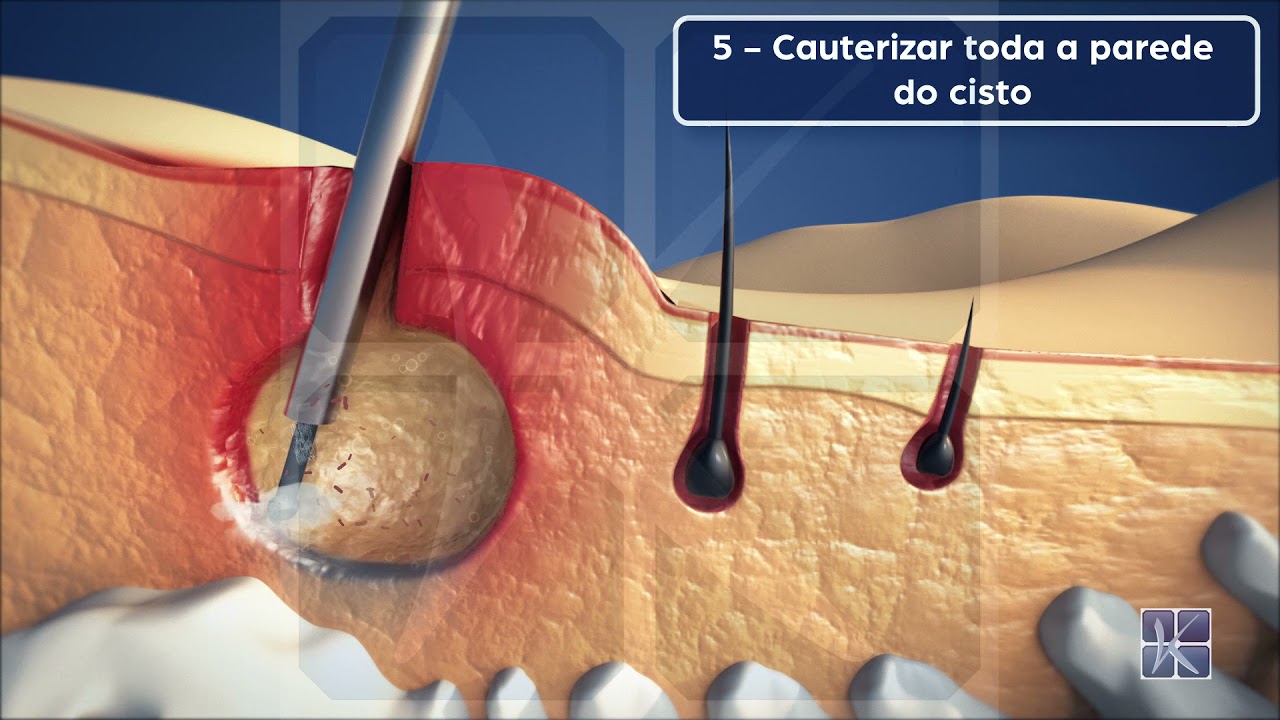
Camera-guided cauterization and cleaning: the entire internal lining of the cyst is destroyed under direct vision. Hair, debris, and necrotic tissue are removed with an endoscopic brush.
Suture of the external opening. No extensive stitches, no open wound. A simple dressing is placed over the entry point.
Same-day discharge — usually 4 to 6 hours after the procedure. The patient goes home walking, accompanied by a companion. Follow-up appointment in 24-48 hours.
Compare the numbers. Understand why patients from around the world choose EPSIT.
| Criteria | EPSIT with Dr. Kaiser Jr. | Conventional Surgery |
|---|---|---|
| Type of incision | 3mm fistuloscope — no external cut | Open cut of 5 to 10 cm |
| Visualization | Direct — HD camera shows entire tract in real time | Indirect — the surgeon cannot see inside the cyst |
| Duration | 20 to 45 minutes | 30 to 60 minutes |
| Anesthesia | Spinal or sedation | General or spinal |
| Hospital stay | Same-day discharge | 1 to 3 days of hospitalization |
| Post-operative dressings | None — simple dressing for 24-48h | Daily, for weeks (open wound) |
| Post-operative pain | Mild — controlled with simple analgesics | Moderate to intense |
| Return to work | 24 to 48 hours | 4 to 8 weeks |
| Return to physical activities | 7 to 14 days (gradual) | 6 to 12 weeks |
| Return to sports | 14 to 30 days | 6 to 12 weeks |
| Scarring | Minimal or none | Significant (5-10 cm) |
| Recurrence | 0 | 20 to 30% |
| Need for reoperation | Rare — technique treats hidden branches | Frequent in recurrent cases |
Dr. Kaiser Jr. brought the EPSIT technique to Brazil and, with over 300 procedures performed, has built the largest case series in the Americas — establishing himself as an international reference in pilonidal cyst treatment.
First surgeon to perform EPSIT in the country. Direct training with the creators of the technique in Europe.
The largest EPSIT case series in Latin America. Volume is one of the main predictors of surgical success.
With a recurrence rate below 10% — significantly better than conventional surgery.
Patients from the USA, Europe, and Latin America travel to be treated by Dr. Kaiser — many after failed conventional surgeries.
Operates at Hospital Albert Einstein (São Paulo), Hospital São Luiz Rede D'Or and at Kaiser Clínica — his own facility designed for One Day Surgery.
Principal Investigator at the Clinical Research Center. Fellow of the Cleveland Clinic (USA) and Universite Louis Pasteur (France).
President of the ROKA Institute for Education and Research. Coordinator of the General Surgery Residency Program.
Real stories from patients who traveled from all over Brazil and abroad to be treated by Dr. Kaiser.

Gabriela
Lived with the cyst for 12 years — same-day discharge
Paolo
Traveled from Texas, USA, to be treated by Dr. Kaiser

Daniel
Came from Florida, USA — definitive solution
The procedure is performed under anesthesia — you feel absolutely nothing during surgery. Post-operative pain is mild and controlled with simple analgesics (dipyrone, acetaminophen). Most patients report minimal discomfort, very different from conventional surgery.
EPSIT (Endoscopic Pilonidal Sinus Treatment) is a minimally invasive endoscopic technique for treating pilonidal cysts. It uses a high-definition camera to visualize and eliminate the cyst from the inside, without the need for large cuts or open incisions.
20 to 45 minutes, depending on the complexity and extent of the fistulous tracts.
No. EPSIT is a Day Surgery (One Day Surgery) procedure. You have surgery in the morning and go home in the afternoon, the same day.
Most patients return to work within 24 to 48 hours for sedentary activities (office, home office). Activities requiring intense physical exertion should wait 7 to 14 days.
EPSIT is especially indicated for recurrent cases. Dr. Kaiser Jr. has extensive experience with patients who have had one or more unsuccessful conventional surgeries. The endoscopic visualization allows identifying tracts and branches that went unnoticed in previous surgery.
The recurrence rate of EPSIT with Dr. Kaiser Jr. is below 10%. This is significantly better than the 20-30% of conventional surgery. Factors such as local hygiene, weight control, and hair removal in the area help prevent recurrence.
The scar is minimal or nonexistent. The fistuloscope is only 3mm — there is no external cut in the skin. The entry opening is so small that it heals spontaneously.
The cost depends on the complexity of the case and the chosen hospital. Some insurance plans cover the procedure — Dr. Kaiser's team provides guidance on coverage and options. Contact us to check.
Yes. Dr. Kaiser Jr. regularly treats patients from all over Brazil and abroad. The team offers telemedicine consultation for initial evaluation, surgical scheduling coordination, travel, accommodation and transport guidance, remote post-operative follow-up, and care in Portuguese, English, and Spanish.
Dr. Kaiser orders standard pre-operative tests (blood work, coagulation panel, cardiac evaluation when indicated). In some cases, an MRI of the sacral region may be requested to map the extent of the tracts.
Yes. Unlike conventional surgery, where sitting is extremely painful for weeks, after EPSIT the discomfort when sitting is minimal. A "donut" cushion can be used for greater comfort in the first 2-3 days.
Yes, EPSIT can treat cysts with multiple fistulous tracts. Endoscopic visualization is precisely the great advantage: it allows identifying and treating each branch. In very extensive cases, Dr. Kaiser may combine EPSIT with other complementary techniques — the decision is always individualized.
Not directly. Sitting for long periods can aggravate the symptoms and make the condition more uncomfortable, but it is not the cause of the cyst. The cause lies in hair penetrating the skin in the intergluteal region.
Hair removal in the intergluteal area can facilitate hygiene and reduce the amount of hair available for skin penetration, but there are no conclusive studies proving it prevents cyst formation. After EPSIT treatment, hair removal may be recommended as an auxiliary measure to reduce the risk of recurrence.
